Breast Augmentation in Plano, TX
“I am so happy with my breast augmentation results! Dr. Friedman is so knowledgeable and meticulous, and he did a great job. You’ll miss out if you don’t go to him.”
- Plano, Texas Breast Augmentation Patient: Cassie
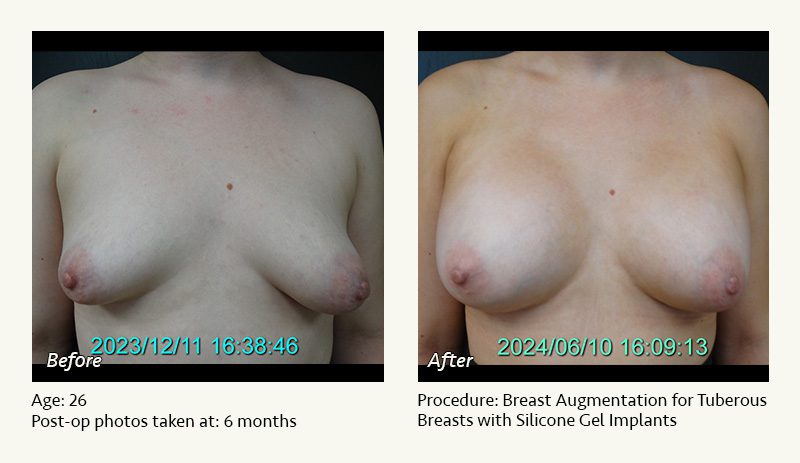
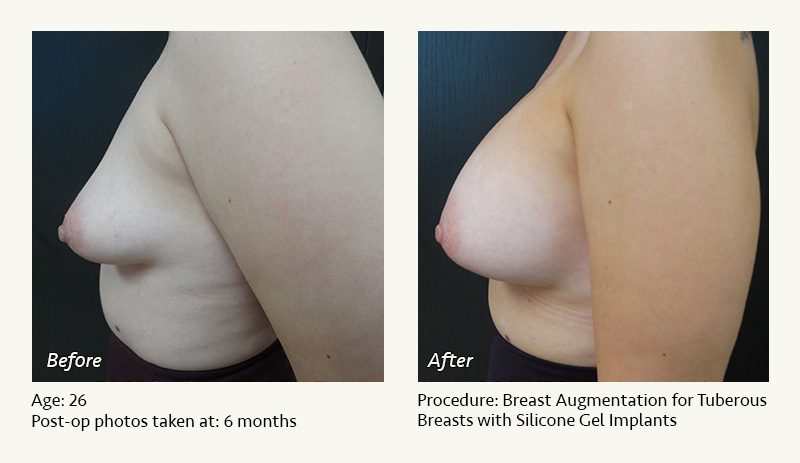
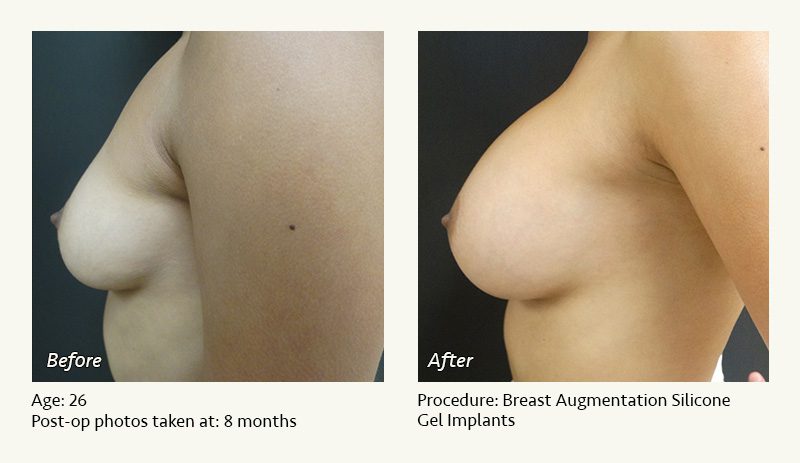
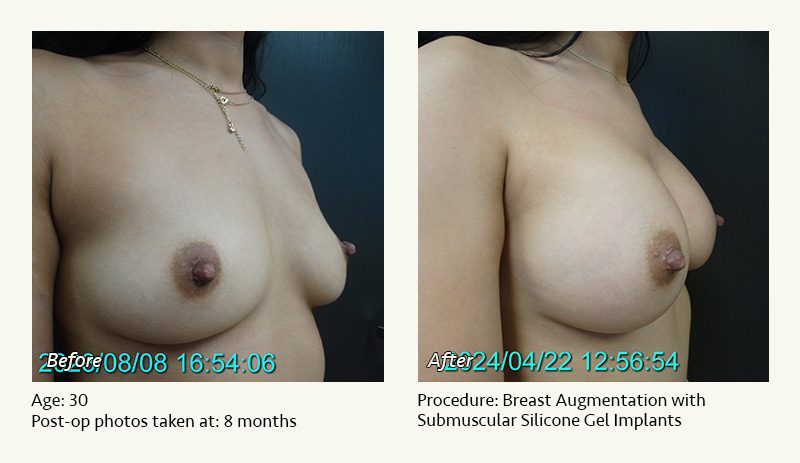
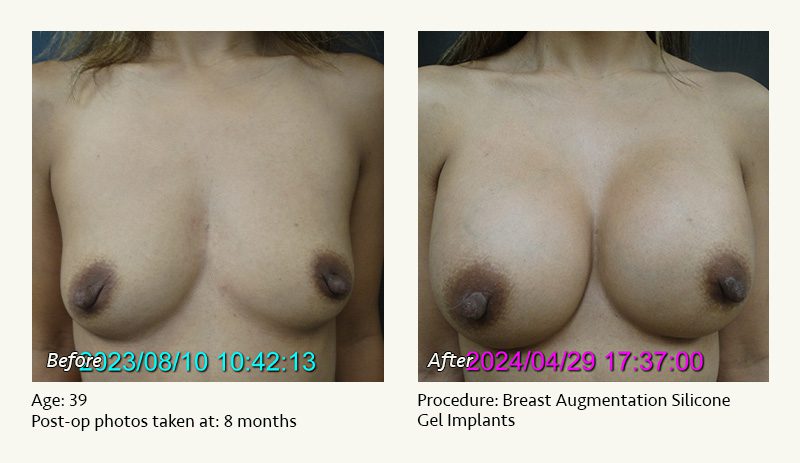
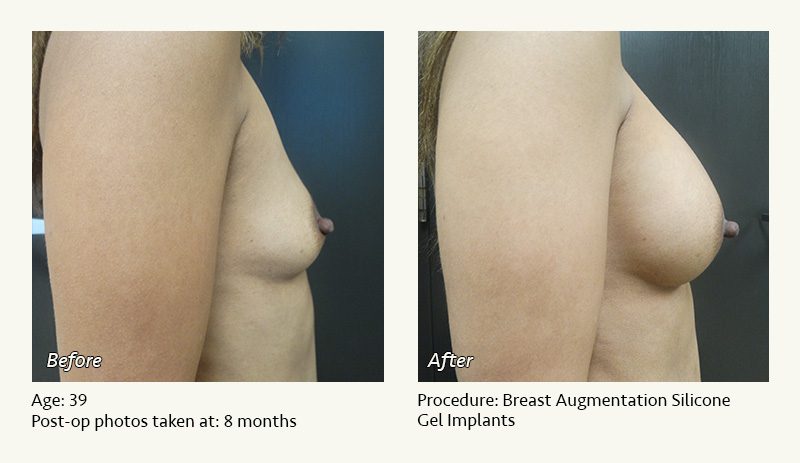
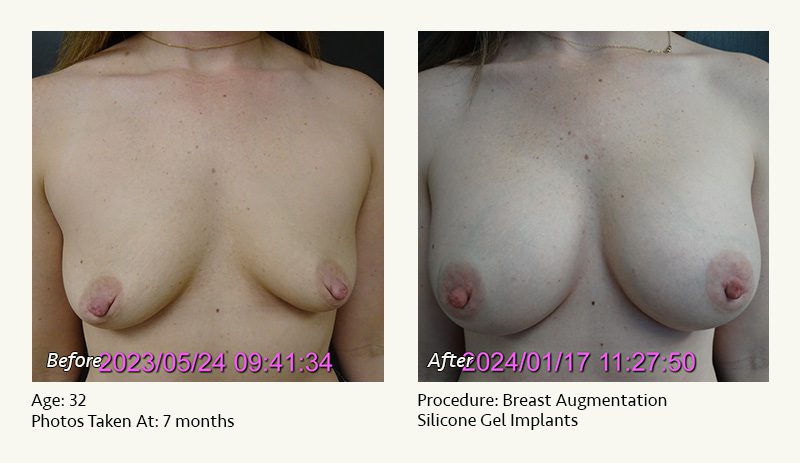
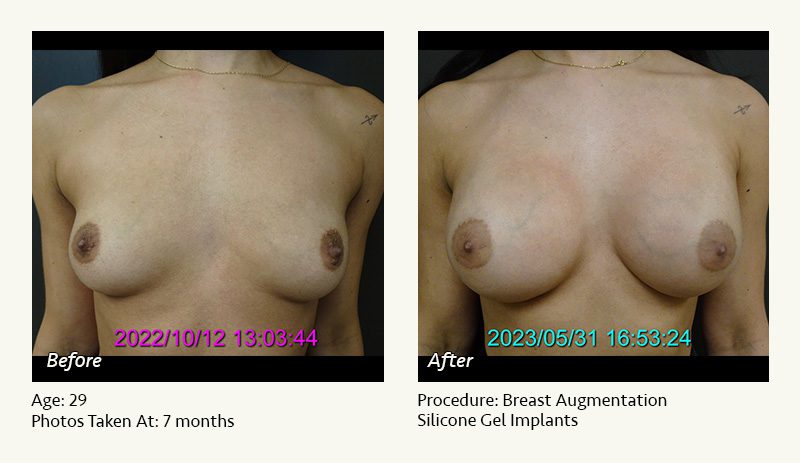
Breast augmentation provides volume, cleavage, and upper breast fullness in women with naturally small breasts or volume loss from pregnancy, weight loss, or aging. Breast augmentation can also provide improved self-image, clothing choices, and confidence.
With 30 years of experience as a wood and marble sculptor, Dr. Friedman in Plano, Texas finds that breast enhancement surgery comes naturally. The average plastic surgeon completes about 35 breast augmentations per year. In contrast, Dr. Friedman performs about 130 breast augmentations annually. Since 1996, he has placed over 5000 breast implants.










































































All About Breast Implants
- Silicone gel vs. saline
- Breast implant size
- Above or below muscle
- Profile, shape, surface, & “gumminess”
Silicone gel vs. saline
Silicone gel breast implants were approved by the FDA in 2006 following many years of study. The FDA temporarily restricted their use in 1992 due to concern regarding possible side effects. There remains no conclusive evidence of a link between silicone gel and any autoimmune disease. Approximately 85% of breast implants currently placed in the U.S. are silicone gel.
Saline-filled breast implants are filled with the salt water solution used in I.V. fluids. If a saline implant leaks, the harmless salt water contents are released and absorbed by the body. Saline implants are covered with a plastic shell made of solid silicone.
Unfortunately, there is no perfect breast implant.

ADVANTAGES OF SILICONE GEL Breast Implants:
- More natural feel. Think jelly, instead of water.
- More natural look. In thin women, silicone gel implants are less likely to produce a visible silhouette along the upper and inner breast.
- Reduced rippling. If you put water in a sandwich bag, you will notice ripples in the bag, just as you will in saline implants.
- Greater durability. Silicone gel implants, on average, have a longer implant lifespan than saline.
ADVANTAGES OF SALINE Breast implants:
- Reduced cost. Saline implants are $1100 less expensive than silicone.
- Smaller incisions. Dr. Friedman in Plano, Texas places saline implants through a 3 cm (just over an inch) incision and places silicone gel implants through an approximately 5 cm (2 inch) incision.
- Reduced risk of capsular contracture (scar tissue causing excessive implant firmness).
- Public perception that it is a “safer” implant. Because ruptures of silicone gel implants may be difficult to detect, the FDA recommends MRI evaluation of silicone implants at regular intervals (every other year) following surgery.
The bottom line: From a purely cosmetic standpoint, silicone gel is probably a better implant than saline. From a medical standpoint, it is difficult to argue with the safety of a bag of salt water. In women with a reasonable amount of breast tissue and subcutaneous fat, Dr. Friedman feels that either saline or silicone gel is a good choice. In women with minimal breast tissue, poor breast tone, and/or minimal subcutaneous fat (and therefore a greater risk for significant rippling with saline implants), silicone gel may be a better choice.
Breast implant size
Determining the “right” breast implant size can be a major challenge.
Let’s discuss the most frequent methods and their pitfalls.
1. Going by bra cup size: “I’m an A cup, and I want to be a full C cup.”
The problem: There is no standardization of cup size among bra manufacturers. A Playtex B is frequently a Victoria’s Secret C. A woman who fits a 34 D cup may also fit a 36 C. So cup size is imprecise, at best, and sometimes closer to a guess.

2. Relying on a surgeon’s determination of the “correct” size based solely on breast measurements.
It has become popular among breast implant surgeons to measure the width of the base of the breast, find an implant with the same diameter (based on a chart provided the implant manufacturers), and then tell the patient that this is the magical “right size.”
The problem: Although this is reasonable anatomically, your desires regarding breast size are much more important than the manufacturer’s or the surgeon’s. While a surgeon can and should provide guidance regarding implant size, the ultimate choice should be yours. If your “right” size is different from his, your surgeon should be flexible (rather than mindlessly following his breast diameter chart).
3. Stuffing your bra with different implant sizes until you find the right one.
This is great for marketing purposes. You get to “try on” different implants until you find the right size.
The problem: The actual implants go under the breast tissues, not over them. Superimposing the implants on top of your breasts creates a snowman effect (one sphere stacked on top of the other), which exaggerates the projection of the breasts relative to what will actually happen in the operating room. Women commonly choose implants that are smaller than they actually wanted.

4. So how do you and Dr. Friedman determine the right implant size?
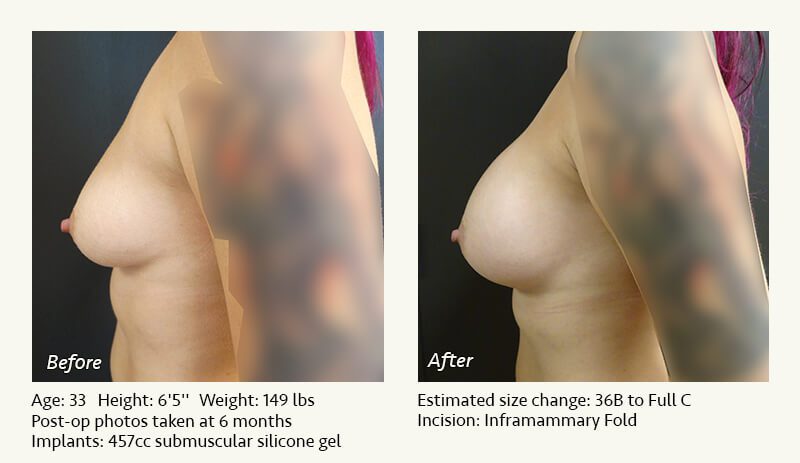
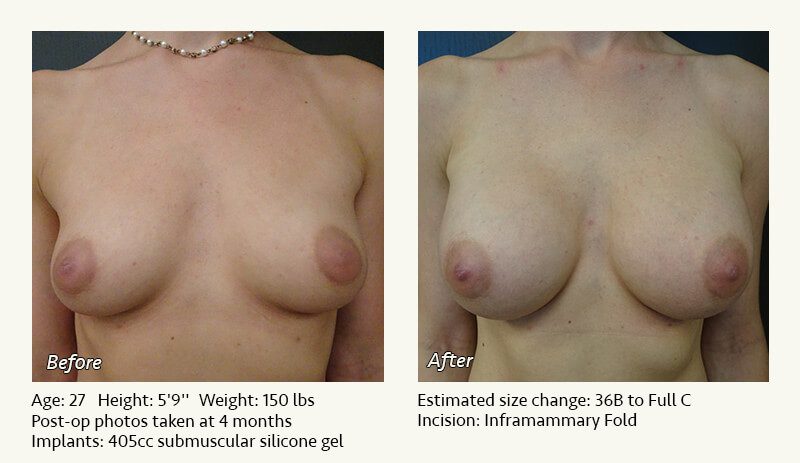
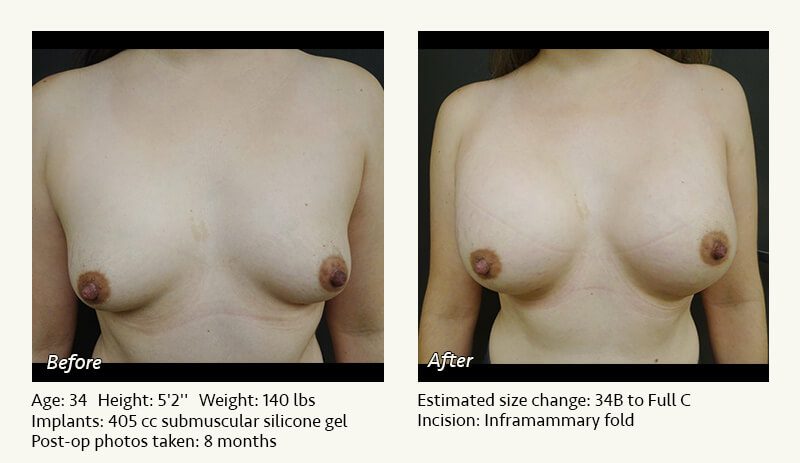
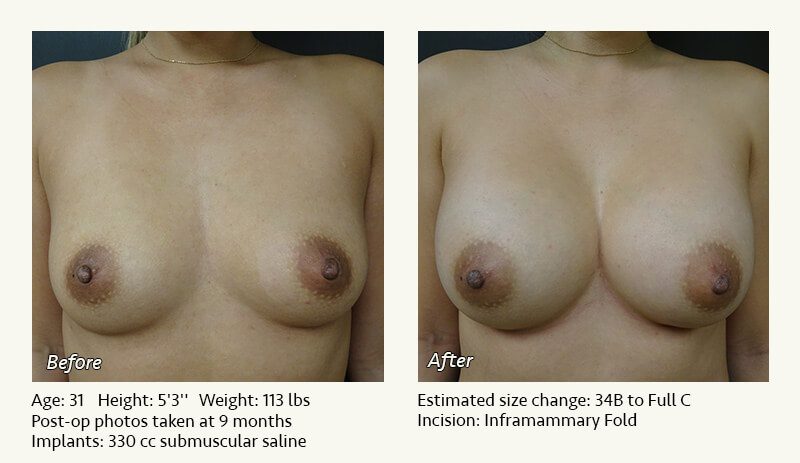
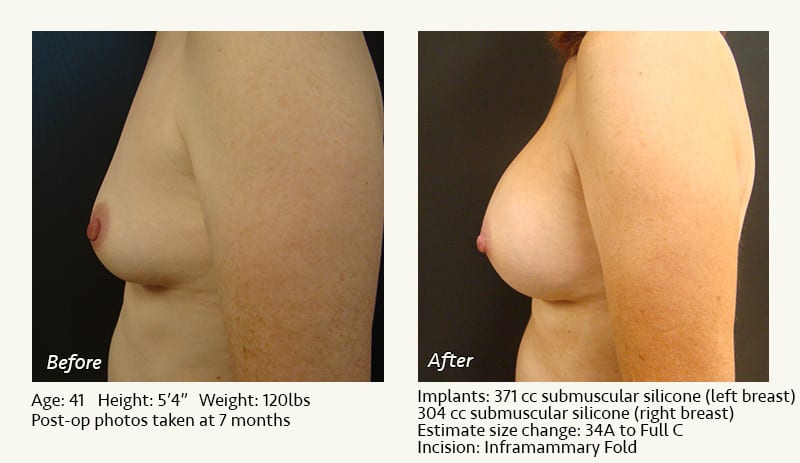
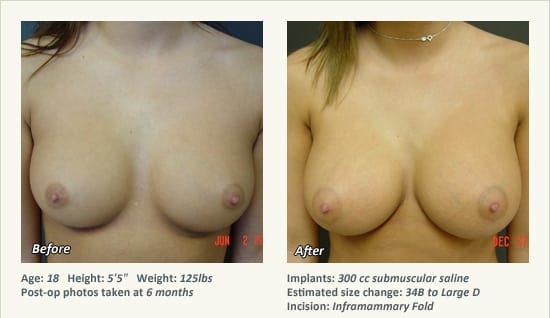
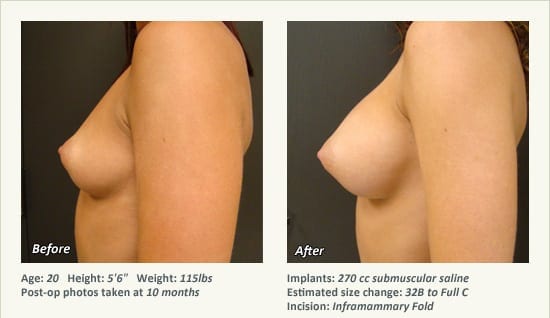
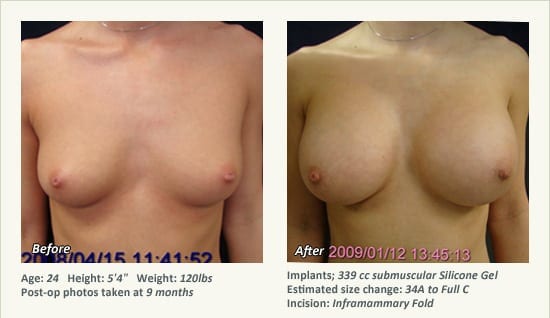
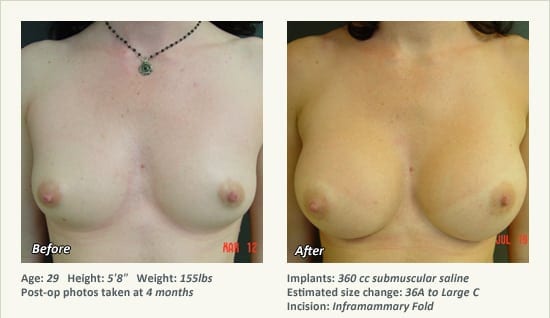
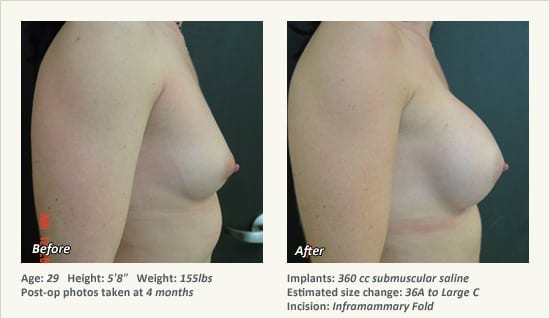
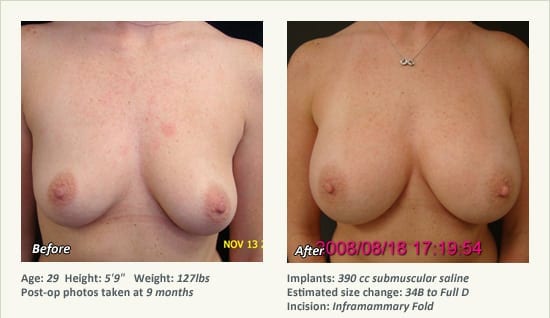
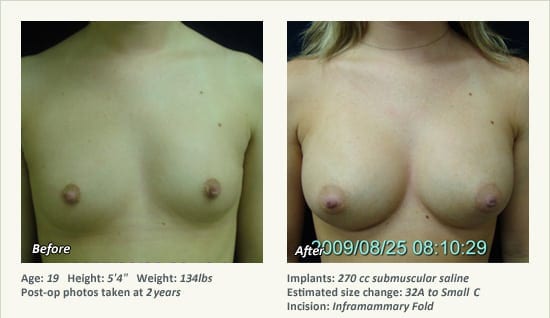
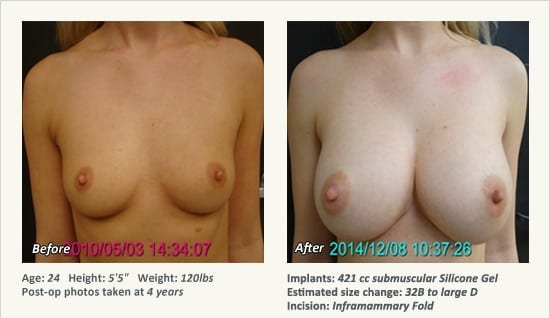
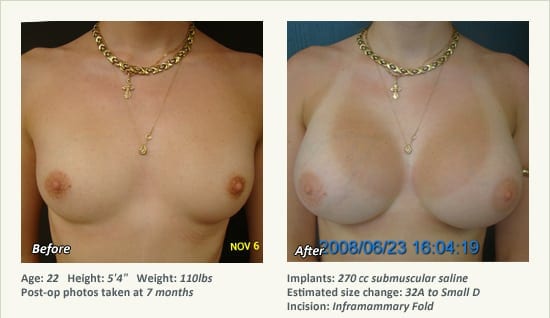
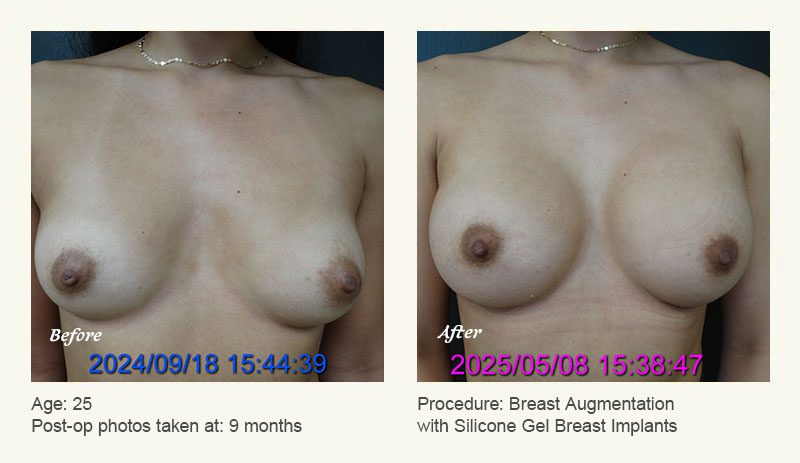
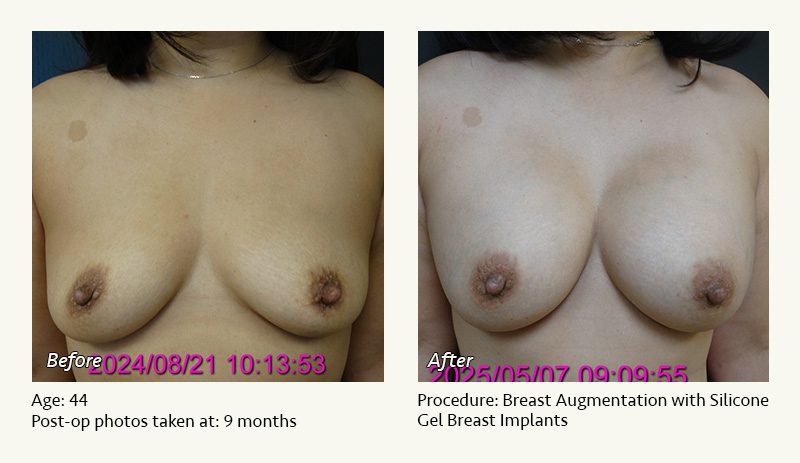
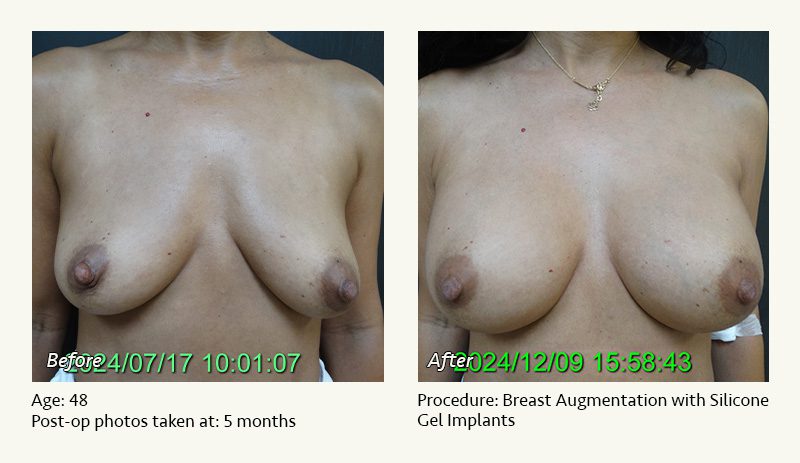
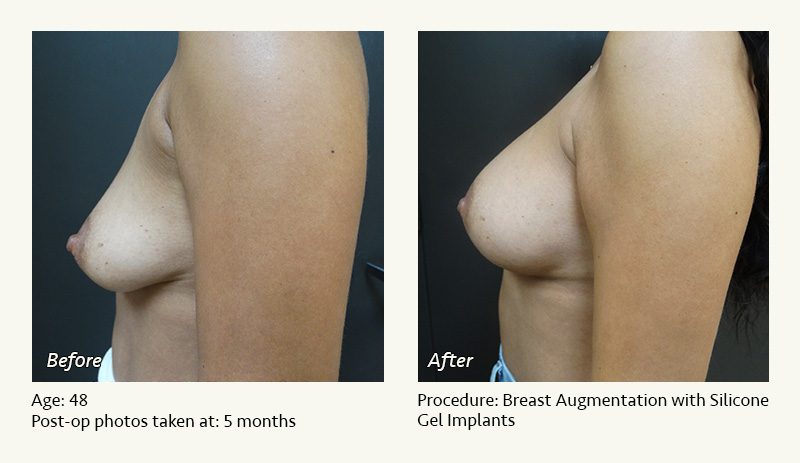
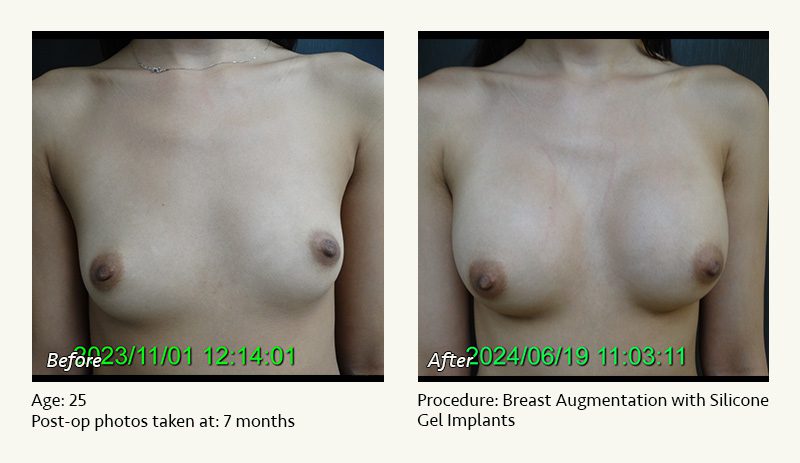
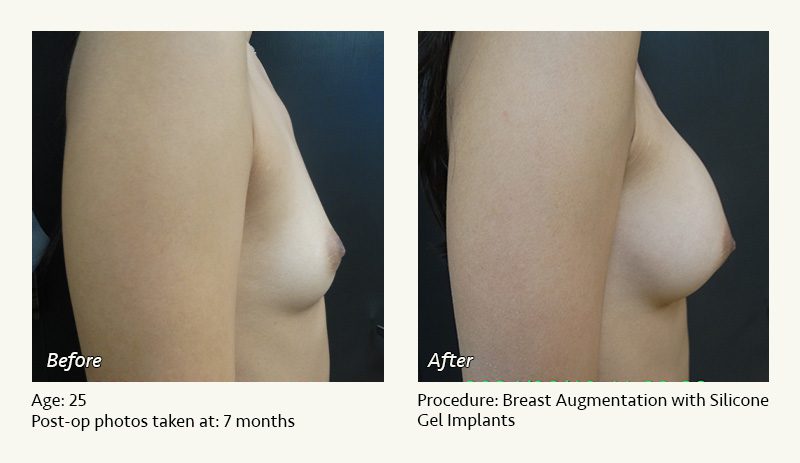
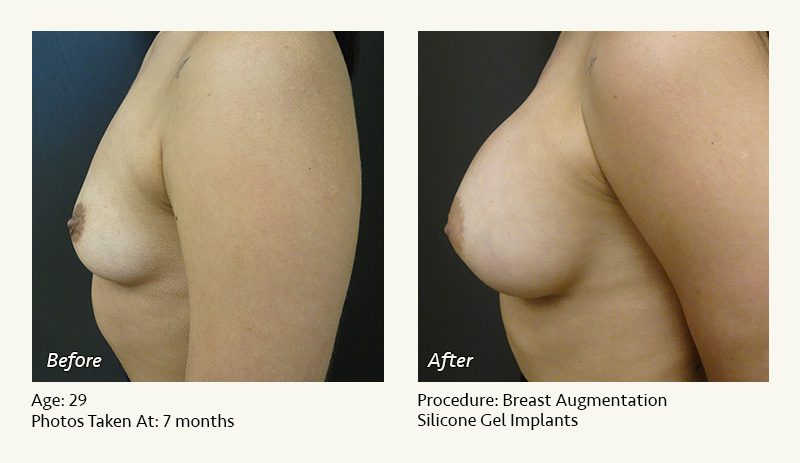
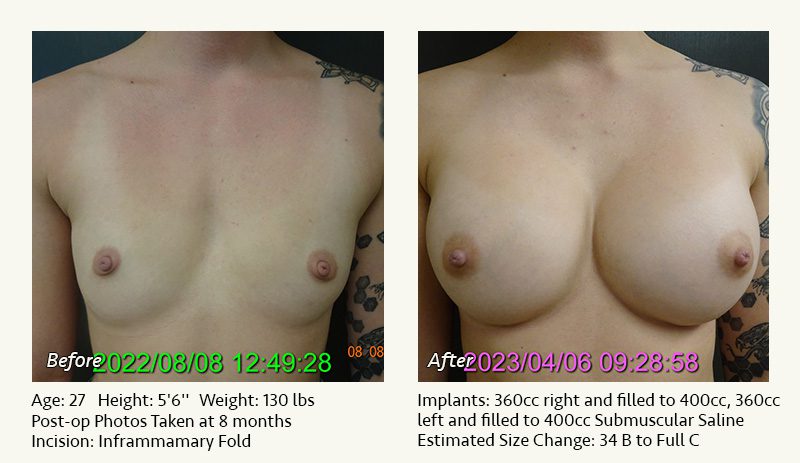
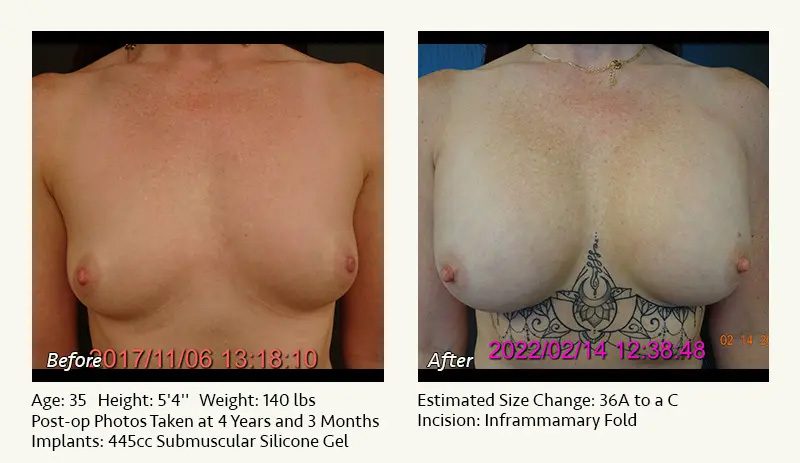
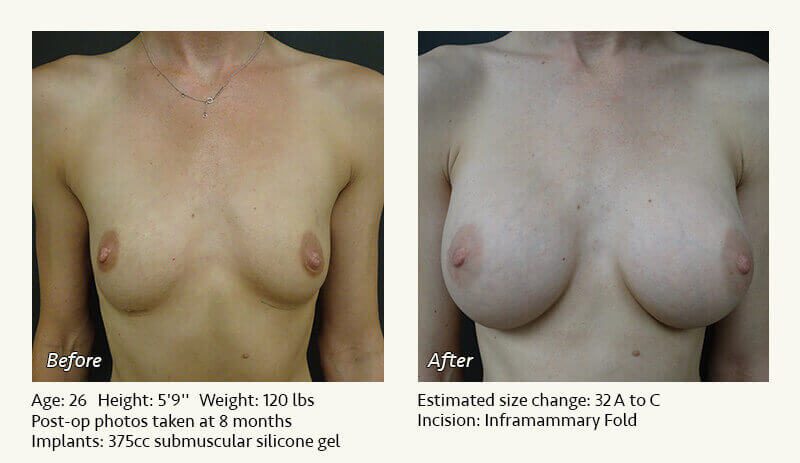
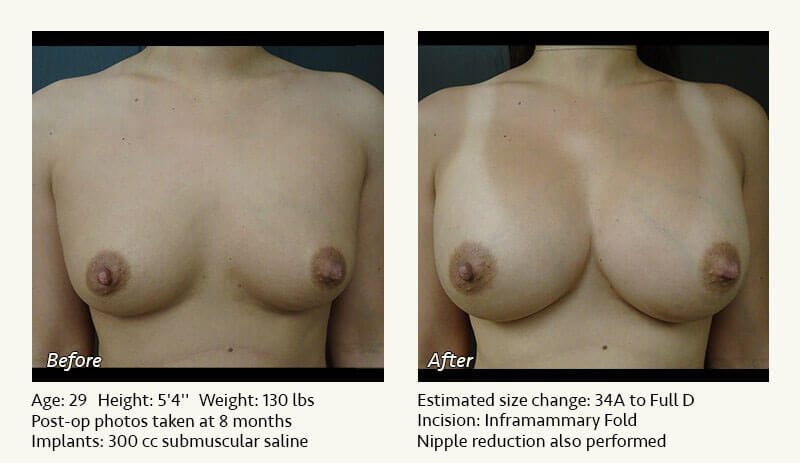
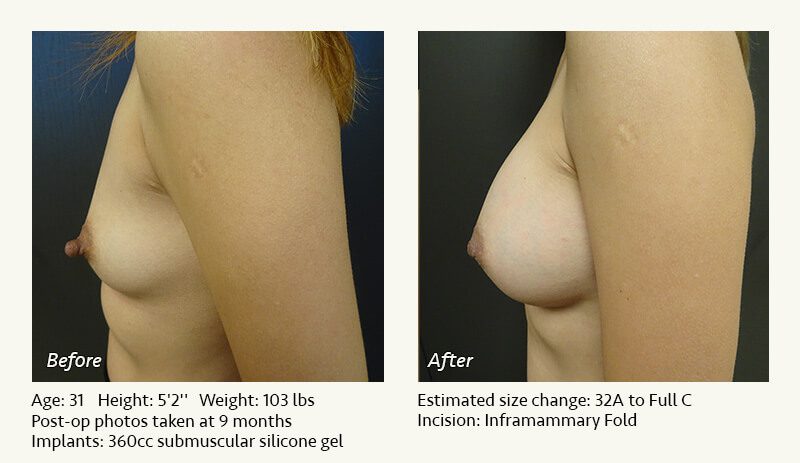
Dr. Friedman in Plano, Texas thinks in terms of implant volumes: 330 cc, 360 cc, 390 cc, etc. You think in terms of cup sizes. Neither of these allows effective communication. So Dr. Friedman uses the one thing that both you and he can see: photos. Although no sizing method works perfectly, photos work better than anything else we have tried.

You can choose among the before and after photos of breast augmentations on our website, among the hundreds of photos in our office photo albums, or among any photos from any magazine or internet site. Although you might not know the cup size of the women you choose or the number of cc’s, it really doesn’t matter. You simply look through breast photos and categorize them as “too big,” “too small,” or “about right.” We will analyze the photos with you. Dr. Friedman believes that there is a range of acceptable sizes, rather than a specific “correct” size.
As long as your photo choices are reasonable for your frame, the choice of breast implant size is yours.
Above or below muscle
Implants can be placed either above (subglandular) or below (submuscular) the pectoralis major muscles.
ADVANTAGES OF SUBMUSCULAR
(BELOW MUSCLE) POSITION:
- Reduced risk of interference with mammography. The muscle separates the implants (below muscle) from the breast tissue (above muscle).
- Reduced risk of capsular contracture (scar tissue causing excessive implant firmness).
- Reduced risk of long-term sagging of the implants. Muscle is more effective than skin in supporting the weight of the implants.
- Reduced rippling of implants. The additional implant coverage provided by the muscle reduces the extent of rippling along the upper and inner breast, particularly with saline implants.
- Reduced risk of a distinct implant silhouette along the upper and inner breasts. The pectoralis major muscle blunts the junction of the upper and inner implant edges and the chest wall.
ADVANTAGES OF SUBGLANDULAR
(ABOVE MUSCLE) POSITION:
- Reduced surgical time, effort, and skill required.
- Reduced discomfort immediately after surgery.
- No risk of weakening the pectoralis major muscles in athletes.
- No implant movement with forceful chest exercise.
The bottom line: Dr. Friedman in Plano, Texas places nearly all breast implants beneath the pectoralis major muscles. He feels strongly that this leads to better long term results in most women. He even published an article about this in Plastic Surgery Practice, a national plastic surgery journal: One Surgeon’s Opinion
Profile, shape, surface, & “gumminess”
Beyond implant size and contents (saline or silicone gel), multiple other variables affect breast implants.
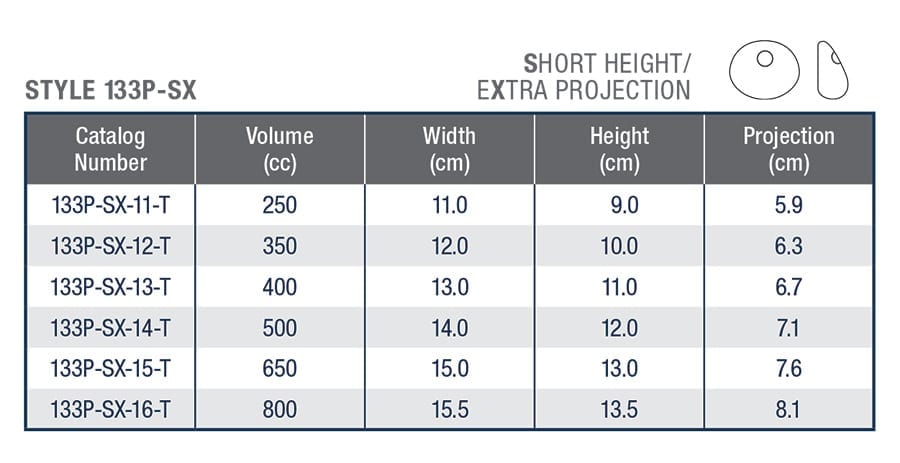
BREAST IMPLANT PROFILE
The profile of a breast implant describes the ratio of the projection of the implant (how far it sticks out) to the diameter of the implant (how wide it is).

In most women seeking augmentation, a moderate or moderate-plus profile breast implant (moderate projection, moderate diameter) provides the most natural look. This is Dr. Friedman’s preference in the vast majority of breast augmentations.
However, in women with narrow chests who desire very large implants, a high profile breast implant (large projection, narrow diameter) may be a reasonable choice, though it may project enough to look a little artificial.
In rare patients who have a wide chest wall and desire a small implant, a low profile breast implant (small projection, large diameter) may be worth consideration.
BREAST IMPLANT SHAPE
Dr. Friedman exclusively uses round breast implants. They accentuate the fullness of the upper breast by equally augmenting the upper and lower breast.
Teardrop or anatomical breast implants preferentially enlarge the lower breast, providing less volume along the upper breast. If a teardrop implant rotates, it distorts the shape of the breast. (If a round implant rotates, breast shape remains unchanged.)

BREAST IMPLANT SURFACE
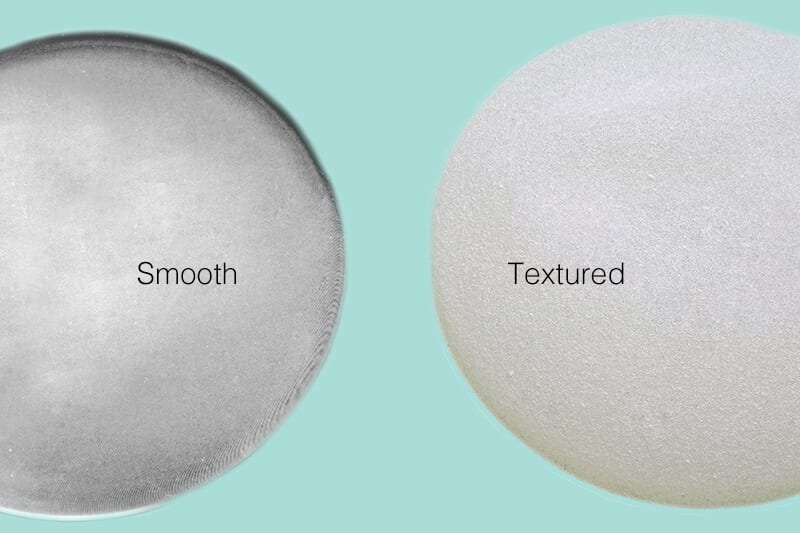
All saline and silicone gel breast implants have an outer shell that is made from solid silicone. As the name implies, smooth implants have a smooth, slick surface. Textured implants have a rough, clingy surface.
Right after breast augmentation surgery, almost all breast implants look too high and too tight. Smooth breast implants are “slippery,” and their weight will cause them to settle after surgery. This is desirable when the implants are below muscle, assuming the pectoralis major muscles have adequate bulk to hold up the implants. Textured breast implants tend to cling to the surrounding tissues. As a result, textured implant are more likely than smooth implants to remain too high and tight on a long term basis. Dr. Friedman limits their use to women whose tissues provide inadequate implant support.
Recent FDA data suggest an association between textured implants and the development of a rare cancer, called breast-implant associated anaplastic large cell lymphoma (BIA-ALCL). No such association has been definitively established for smooth implants.
For these reasons, Dr. Friedman uses smooth breast implants in over 99% of his breast augmentation patients.
Breast Implant “Gumminess”
Saline implants are filled with saltwater. They are never “gummy”. Silicone gel implants are more viscous or jelly-like, so they feel more like breast tissues. The viscosity or thickness of silicone gel implants varies; the firmer the material, the “gummier” the implant.
Silicone gel implants manufactured by Allergan are available in three levels of viscosity:
| Responsive | Smooth Touch | Cohesive | |
| Firmness | Softer | Moderate | Firmer |
| Rippling | Greater | Moderate | Lesser |
| Incision | Shorter | Moderate | Longer |
| Price | Lower | Moderate | Higher |
For most women seeking silicone gel augmentation, Dr. Friedman recommends the Responsive implants. These feel the softest (most natural), are the least expensive, and require the smallest incision. However, in women with very thin tissues (particularly those whose tissues are stretched due to prior augmentation surgery), he may recommend Smooth Touch or Cohesive implants due to their lower risk of surface rippling.
Silicone gel vs. saline
Silicone gel vs. saline
Silicone gel breast implants were approved by the FDA in 2006 following many years of study. The FDA temporarily restricted their use in 1992 due to concern regarding possible side effects. There remains no conclusive evidence of a link between silicone gel and any autoimmune disease. Approximately 85% of breast implants currently placed in the U.S. are silicone gel.
Saline-filled breast implants are filled with the salt water solution used in I.V. fluids. If a saline implant leaks, the harmless salt water contents are released and absorbed by the body. Saline implants are covered with a plastic shell made of solid silicone.
Unfortunately, there is no perfect breast implant.
ADVANTAGES OF SILICONE GEL Breast Implants:
- More natural feel. Think jelly, instead of water.
- More natural look. In thin women, silicone gel implants are less likely to produce a visible silhouette along the upper and inner breast.
- Reduced rippling. If you put water in a sandwich bag, you will notice ripples in the bag, just as you will in saline implants.
- Greater durability. Silicone gel implants, on average, have a longer implant lifespan than saline.
ADVANTAGES OF SALINE Breast implants:
- Reduced cost. Saline implants are $1100 less expensive than silicone.
- Smaller incisions. Dr. Friedman in Plano, Texas places saline implants through a 3 cm (just over an inch) incision and places silicone gel implants through an approximately 5 cm (2 inch) incision.
- Reduced risk of capsular contracture (scar tissue causing excessive implant firmness).
- Public perception that it is a “safer” implant. Because ruptures of silicone gel implants may be difficult to detect, the FDA recommends MRI evaluation of silicone implants at regular intervals (every other year) following surgery.
The bottom line: From a purely cosmetic standpoint, silicone gel is probably a better implant than saline. From a medical standpoint, it is difficult to argue with the safety of a bag of salt water. In women with a reasonable amount of breast tissue and subcutaneous fat, Dr. Friedman feels that either saline or silicone gel is a good choice. In women with minimal breast tissue, poor breast tone, and/or minimal subcutaneous fat (and therefore a greater risk for significant rippling with saline implants), silicone gel may be a better choice.
Close
Breast implant size
Breast implant size
Determining the “right” breast implant size can be a major challenge.
Let’s discuss the most frequent methods and their pitfalls.
1. Going by bra cup size: “I’m an A cup, and I want to be a full C cup.”
The problem: There is no standardization of cup size among bra manufacturers. A Playtex B is frequently a Victoria’s Secret C. A woman who fits a 34 D cup may also fit a 36 C. So cup size is imprecise, at best, and sometimes closer to a guess.
2. Relying on a surgeon’s determination of the “correct” size based solely on breast measurements.
It has become popular among breast implant surgeons to measure the width of the base of the breast, find an implant with the same diameter (based on a chart provided the implant manufacturers), and then tell the patient that this is the magical “right size.”
The problem: Although this is reasonable anatomically, your desires regarding breast size are much more important than the manufacturer’s or the surgeon’s. While a surgeon can and should provide guidance regarding implant size, the ultimate choice should be yours. If your “right” size is different from his, your surgeon should be flexible (rather than mindlessly following his breast diameter chart).
3. Stuffing your bra with different implant sizes until you find the right one.
This is great for marketing purposes. You get to “try on” different implants until you find the right size.
The problem: The actual implants go under the breast tissues, not over them. Superimposing the implants on top of your breasts creates a snowman effect (one sphere stacked on top of the other), which exaggerates the projection of the breasts relative to what will actually happen in the operating room. Women commonly choose implants that are smaller than they actually wanted.
4. So how do you and Dr. Friedman determine the right implant size?
Dr. Friedman in Plano, Texas thinks in terms of implant volumes: 330 cc, 360 cc, 390 cc, etc. You think in terms of cup sizes. Neither of these allows effective communication. So Dr. Friedman uses the one thing that both you and he can see: photos. Although no sizing method works perfectly, photos work better than anything else we have tried.
You can choose among the before and after photos of breast augmentations on our website, among the hundreds of photos in our office photo albums, or among any photos from any magazine or internet site. Although you might not know the cup size of the women you choose or the number of cc’s, it really doesn’t matter. You simply look through breast photos and categorize them as “too big,” “too small,” or “about right.” We will analyze the photos with you. Dr. Friedman believes that there is a range of acceptable sizes, rather than a specific “correct” size.
As long as your photo choices are reasonable for your frame, the choice of breast implant size is yours.
Close
Above or below muscle
Above or below muscle
Implants can be placed either above (subglandular) or below (submuscular) the pectoralis major muscles.
ADVANTAGES OF SUBMUSCULAR
(BELOW MUSCLE) POSITION:
- Reduced risk of interference with mammography. The muscle separates the implants (below muscle) from the breast tissue (above muscle).
- Reduced risk of capsular contracture (scar tissue causing excessive implant firmness).
- Reduced risk of long-term sagging of the implants. Muscle is more effective than skin in supporting the weight of the implants.
- Reduced rippling of implants. The additional implant coverage provided by the muscle reduces the extent of rippling along the upper and inner breast, particularly with saline implants.
- Reduced risk of a distinct implant silhouette along the upper and inner breasts. The pectoralis major muscle blunts the junction of the upper and inner implant edges and the chest wall.
ADVANTAGES OF SUBGLANDULAR
(ABOVE MUSCLE) POSITION:
- Reduced surgical time, effort, and skill required.
- Reduced discomfort immediately after surgery.
- No risk of weakening the pectoralis major muscles in athletes.
- No implant movement with forceful chest exercise.
The bottom line: Dr. Friedman in Plano, Texas places nearly all breast implants beneath the pectoralis major muscles. He feels strongly that this leads to better long term results in most women. He even published an article about this in Plastic Surgery Practice, a national plastic surgery journal: One Surgeon’s Opinion
Close
Profile, shape, surface, & “gumminess”
Profile, shape, surface, & “gumminess”
Beyond implant size and contents (saline or silicone gel), multiple other variables affect breast implants.
BREAST IMPLANT PROFILE
The profile of a breast implant describes the ratio of the projection of the implant (how far it sticks out) to the diameter of the implant (how wide it is).
In most women seeking augmentation, a moderate or moderate-plus profile breast implant (moderate projection, moderate diameter) provides the most natural look. This is Dr. Friedman’s preference in the vast majority of breast augmentations.
However, in women with narrow chests who desire very large implants, a high profile breast implant (large projection, narrow diameter) may be a reasonable choice, though it may project enough to look a little artificial.
In rare patients who have a wide chest wall and desire a small implant, a low profile breast implant (small projection, large diameter) may be worth consideration.
BREAST IMPLANT SHAPE
Dr. Friedman exclusively uses round breast implants. They accentuate the fullness of the upper breast by equally augmenting the upper and lower breast.
Teardrop or anatomical breast implants preferentially enlarge the lower breast, providing less volume along the upper breast. If a teardrop implant rotates, it distorts the shape of the breast. (If a round implant rotates, breast shape remains unchanged.)
BREAST IMPLANT SURFACE
All saline and silicone gel breast implants have an outer shell that is made from solid silicone. As the name implies, smooth implants have a smooth, slick surface. Textured implants have a rough, clingy surface.
Right after breast augmentation surgery, almost all breast implants look too high and too tight. Smooth breast implants are “slippery,” and their weight will cause them to settle after surgery. This is desirable when the implants are below muscle, assuming the pectoralis major muscles have adequate bulk to hold up the implants. Textured breast implants tend to cling to the surrounding tissues. As a result, textured implant are more likely than smooth implants to remain too high and tight on a long term basis. Dr. Friedman limits their use to women whose tissues provide inadequate implant support.
Recent FDA data suggest an association between textured implants and the development of a rare cancer, called breast-implant associated anaplastic large cell lymphoma (BIA-ALCL). No such association has been definitively established for smooth implants.
For these reasons, Dr. Friedman uses smooth breast implants in over 99% of his breast augmentation patients.
Breast Implant “Gumminess”
Saline implants are filled with saltwater. They are never “gummy”. Silicone gel implants are more viscous or jelly-like, so they feel more like breast tissues. The viscosity or thickness of silicone gel implants varies; the firmer the material, the “gummier” the implant.
Silicone gel implants manufactured by Allergan are available in three levels of viscosity:
| Responsive | Smooth Touch | Cohesive | |
| Firmness | Softer | Moderate | Firmer |
| Rippling | Greater | Moderate | Lesser |
| Incision | Shorter | Moderate | Longer |
| Price | Lower | Moderate | Higher |
For most women seeking silicone gel augmentation, Dr. Friedman recommends the Responsive implants. These feel the softest (most natural), are the least expensive, and require the smallest incision. However, in women with very thin tissues (particularly those whose tissues are stretched due to prior augmentation surgery), he may recommend Smooth Touch or Cohesive implants due to their lower risk of surface rippling.
Close
Why choose Dr. Friedman for your breast augmentation?
Dr. Friedman in Plano, Texas performs an average of over 100 breast augmentations annually (vs. about 35 for the average plastic surgeon), and he has been in practice for well over 25 years. He has placed over 5000 breast implants.
Beyond his decades of experience as a plastic surgeon and wood and marble sculptor, before-and-after results, and outstanding patient reviews, here are some important reasons to choose Dr. Friedman for your breast augmentation:
Surgical technique
- Most surgeons perform breast augmentation using a technique called “blunt dissection.” They use a blunt instrument or a gloved finger to tear the pectoralis major muscle off the ribs. Then they put in your breast implants. Blunt dissection is fast. (Some surgeons can complete your procedure in less than 30 minutes.) Unfortunately, it causes significant tissue trauma and bleeding and may lead to increased complication rates and reoperations. To reduce bleeding, many surgeons use surgical drainage tubes, compression bras, and/or ACE bandages following surgery.In contrast, Dr. Friedman uses electrocautery to perform your surgery. This involves use of a thin, long, matchstick-shaped instrument that heat-seals the tissues as they are elevated. This reduces bleeding (Dr. Friedman’s average blood loss is under an ounce), virtually eliminates bruising, and makes drainage tubes, ACE bandages, and compression bras unnecessary.
- Most surgeons “release” the pectoralis major muscles by cutting the entire lower portions in half to accommodate the implants. This frequently results in excessive descent or “bottoming out” of the breast implants in the months and years following surgery.In contrast, Dr. Friedman releases little or none of the pectoralis major muscles in most women. A largely intact pectoralis major provides better implant support and “perkier” long-term results.
- Most surgeons choose implant size based on dimensional charts from implant manufacturers or based on women “trying on” sample breast implants. Neither of these methods works particularly well.In contrast, Dr. Friedman encourages you to choose photos of women with the breast size you desire. After creating “pockets” for your implants, Dr. Friedman places “sizers,” which are sterile sample implants, and temporarily sits you up on the operating table (while you are asleep under anesthesia). This enables him to preview and adjust your results before selecting the implants that best match your anatomy and the photos of desired size that you have chosen.
These technical modifications add time to the surgery. But they provide improved results and reduced complication and reoperation rates. Dr. Friedman looks at it this way: “It may be a couple hours out of my life, but it’s the rest of yours.”
Safety
Your safety is our highest priority.
- Your outpatient surgery will be performed under general anesthesia at the West Plano Plastic Surgery Center, which has been nationally accredited by the American Association for the Accreditation of Ambulatory Surgical Facilities (AAAASF) since the year 2000. Dr. Friedman is the Founder and Director of the Center. AAAASF has stringent accreditation standards and requires regular inspections and annual recertification.
- The West Plano Plastic Surgery Center is located immediately adjacent to Dr. Friedman’s office in Professional Medical Building 3 at Texas Health Presbyterian Hospital of Plano. You will not be in a freestanding surgery center miles from a hospital; you will be on the campus of one of the premier hospitals in North Texas.
- Unlike most plastic surgeons, Dr. Friedman exclusively uses physician anesthesiologists—not nurses or technicians—to administer your anesthesia. He believes that their superior training provides a safer patient experience.
Artistry
Unlike the vast majority of surgeons who claim that they can “sculpt” your breasts, Dr. Friedman is actually an experienced and respected wood and marble sculptor whose work has been displayed in galleries and is part of many private collections. He was an accomplished artist well before he attended medical school. For Dr. Friedman, breast and body contouring surgery represents the synthesis of his talents as an artist and a plastic surgeon.
- Before


- After

Torso carved from Nepalese rosewood
by Ronald M. Friedman, M.D.
Please click here to view photos of Dr. Friedman’s wood and marble sculptures.
Surgical technique
Surgical technique
- Most surgeons perform breast augmentation using a technique called “blunt dissection.” They use a blunt instrument or a gloved finger to tear the pectoralis major muscle off the ribs. Then they put in your breast implants. Blunt dissection is fast. (Some surgeons can complete your procedure in less than 30 minutes.) Unfortunately, it causes significant tissue trauma and bleeding and may lead to increased complication rates and reoperations. To reduce bleeding, many surgeons use surgical drainage tubes, compression bras, and/or ACE bandages following surgery.In contrast, Dr. Friedman uses electrocautery to perform your surgery. This involves use of a thin, long, matchstick-shaped instrument that heat-seals the tissues as they are elevated. This reduces bleeding (Dr. Friedman’s average blood loss is under an ounce), virtually eliminates bruising, and makes drainage tubes, ACE bandages, and compression bras unnecessary.
- Most surgeons “release” the pectoralis major muscles by cutting the entire lower portions in half to accommodate the implants. This frequently results in excessive descent or “bottoming out” of the breast implants in the months and years following surgery.In contrast, Dr. Friedman releases little or none of the pectoralis major muscles in most women. A largely intact pectoralis major provides better implant support and “perkier” long-term results.
- Most surgeons choose implant size based on dimensional charts from implant manufacturers or based on women “trying on” sample breast implants. Neither of these methods works particularly well.In contrast, Dr. Friedman encourages you to choose photos of women with the breast size you desire. After creating “pockets” for your implants, Dr. Friedman places “sizers,” which are sterile sample implants, and temporarily sits you up on the operating table (while you are asleep under anesthesia). This enables him to preview and adjust your results before selecting the implants that best match your anatomy and the photos of desired size that you have chosen.
These technical modifications add time to the surgery. But they provide improved results and reduced complication and reoperation rates. Dr. Friedman looks at it this way: “It may be a couple hours out of my life, but it’s the rest of yours.”
Close
Safety
Safety
Your safety is our highest priority.
- Your outpatient surgery will be performed under general anesthesia at the West Plano Plastic Surgery Center, which has been nationally accredited by the American Association for the Accreditation of Ambulatory Surgical Facilities (AAAASF) since the year 2000. Dr. Friedman is the Founder and Director of the Center. AAAASF has stringent accreditation standards and requires regular inspections and annual recertification.
- The West Plano Plastic Surgery Center is located immediately adjacent to Dr. Friedman’s office in Professional Medical Building 3 at Texas Health Presbyterian Hospital of Plano. You will not be in a freestanding surgery center miles from a hospital; you will be on the campus of one of the premier hospitals in North Texas.
- Unlike most plastic surgeons, Dr. Friedman exclusively uses physician anesthesiologists—not nurses or technicians—to administer your anesthesia. He believes that their superior training provides a safer patient experience.
Close
Artistry
Artistry
Unlike the vast majority of surgeons who claim that they can “sculpt” your breasts, Dr. Friedman is actually an experienced and respected wood and marble sculptor whose work has been displayed in galleries and is part of many private collections. He was an accomplished artist well before he attended medical school. For Dr. Friedman, breast and body contouring surgery represents the synthesis of his talents as an artist and a plastic surgeon.
- Before
- After
Torso carved from Nepalese rosewood
by Ronald M. Friedman, M.D.
Please click here to view photos of Dr. Friedman’s wood and marble sculptures.
Close
When you visit our office in Plano, Texas, we will be happy to show you a variety of “before and after” photos of breast enlargements performed by Dr. Friedman. You will also be able to see and feel the differences between saline and silicone gel implants. If you wish to speak to other women who have undergone breast augmentation, we will be happy to provide phone numbers.


Q & A: Breast Augmentation
-
Do most women choose silicone gel or saline breast implants?
Approximately 90% of breast implants currently placed in the United States are silicone gel. Saline implants remain a reasonable alternative, particularly in women with a significant amount of breast tissue and subcutaneous fat.
-
Are there any restrictions on the use of silicone gel breast implants?
The FDA has restricted the use of silicone gel implants to women ages 22 and greater except in the case of severe breast developmental deformities. For women ages 18 to 21, saline implants remain a viable alternative.
-
How long will my breast implants last?
Your implants will probably not last as long as you do. It is likely that one or both of your implants will require replacement at some point in your lifetime due to deflation (saline) or rupture (silicone gel). Most saline implants will last at least 10 years; most silicone gel implants will last at least 15 years. In the absence of an implant-related problem, there is no need to “change out” your implants (i.e. if it isn’t broken, don’t fix it).
-
Are ruptured breast implants dangerous?
Saline implants are filled with sterile saltwater. Upon deflation, the saline is absorbed harmlessly. There is no known health risk associated with deflated saline implants. The FDA has determined that intact silicone gel implants are safe. However, they have not made a determination regarding the safety of ruptured silicone gel implants. Therefore, the FDA currently recommends that any ruptured silicone gel implant be removed.
-
Where are the incisions located?
Dr. Friedman performs breast augmentation through an inframammary approach, using incisions located near the creases beneath the breasts. Typical incisions are 3 cm (just over an inch) for saline and approximately 5 cm (2 inches) for silicone gel. Incisions around the nipple-areolae (periareolar approach) are associated with a greater risk of infection, capsular contracture, and interference with breastfeeding. Incisions in the armpits (axillary approach) are associated with a high risk of capsular contracture and an increased risk of implant malposition.
-
How much cleavage I will have after breast augmentation?
Your cleavage after surgery is determined by the following factors:
- Your anatomy. Regardless of your breast size, you can probably look at your breasts in the mirror and see whether they are close together (figure 1) or far apart (figure 2). The distance between your breasts before surgery strongly influences the distance between your breasts after surgery.

 Figure 1: More cleavage before surgery–and after surgery.
Figure 1: More cleavage before surgery–and after surgery.
 Figure 2: Less cleavage before surgery–and after surgery.
Figure 2: Less cleavage before surgery–and after surgery. - Implant size. In general, larger implants create more cleavage than smaller implants. More specifically, implants with a larger diameter extend closer to the midline than those with a smaller diameter. If cleavage is a major priority, then use the largest implant with which you feel comfortable.
- Surgical technique. Dr. Friedman routinely places breast implants under the pectoralis major muscles (see above). Having done this operation thousands of times, he has noticed that the pectoralis muscles have an outer leaflet (further from the midline) and an inner leaflet (closer to the midline). Dr. Friedman frequently divides the outer leaflet to maximize cleavage—while preserving the integrity of the inner leaflet.
- Your anatomy. Regardless of your breast size, you can probably look at your breasts in the mirror and see whether they are close together (figure 1) or far apart (figure 2). The distance between your breasts before surgery strongly influences the distance between your breasts after surgery.
-
What are “gummy bear” breast implants?
All silicone gel implants are “cohesive,” meaning that silicone is a viscous material (like molasses). Some implants are more cohesive than others. Highly cohesive implants have informally been called “gummy bears.” Their advantages include reduced implant rippling (particularly in thin women with minimal breast tissue who are undergoing revision augmentation surgery) and reduced implant gel dispersion with rupture. Their disadvantages include mildly longer incisions and significantly increased cost.
For more detailed information about gummy bear implants, please click here.
-
Can breast implants interfere with mammograms?
Implants may reduce the sensitivity of mammograms. This is a greater concern for implants placed above muscle than those placed below muscle. In order to better visualize the breast tissues, additional mammography views (such as the Eklund displacement view) are recommended. Of interest, implants may actually make it easier to detect breast lumps on physical exam.
-
Does Dr. Friedman do breast implant revision surgery?
Approximately 20% of the roughly 140 breast augmentations performed by Dr. Friedman annually are breast implant revisions. Many of these women are referred by other physicians. Dr. Friedman performs revisions to increase or decrease implant size, remove and replace deflated or ruptured implants, soften breasts that have become hard (capsular contracture), or improve breast implant position and shape.
-
Can breast augmentation be combined with other procedures?
Dr. Friedman frequently performs breast augmentation with breast lift in women who desire improvement in breast sagging from pregnancy, weight loss, or aging. He also performs a large number of mommy makeover procedures, combining breast augmentation with liposuction and/or tummy tuck.